Agri-Health Webinar Series: What We Learned About Food is Medicine

This blog is the first in a series of five session summaries from the Agri-Health webinar series, made possible through the EIP “Collaborating on Innovation” grant from the Province of South Holland and the European Union. Within the AHOPM consortium, we are developing a new model that integrates agriculture, healthcare, and impact finance. Our goal is to embed healthy food structurally within healthcare systems, while creating new markets for organic and regenerative farmers.
For this first session, we welcomed Dr Ronit Ridberg from the Food is Medicine Institute at Tufts University. The institute integrates research, policy, and education to advance the practical implementation of Food is Medicine. During the webinar, Dr Ridberg provided an overview of how the field is evolving, the current scientific evidence, and the key questions involved in translating these models to other contexts, including Europe and the Netherlands.
1. Food is Medicine as a healthcare approach
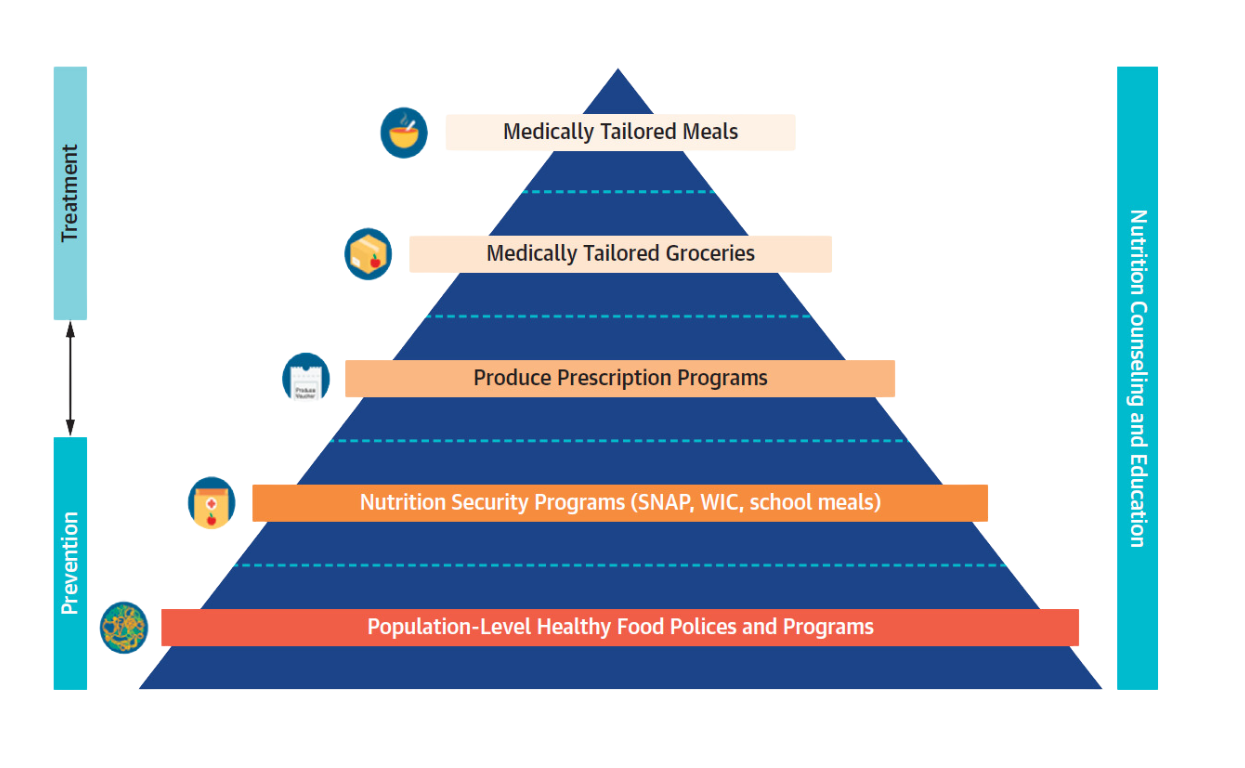
Food is Medicine refers to programs and interventions that support and promote healthy dietary patterns to prevent and treat diet-related conditions. This is done by providing access to nutritious food that is fully or partially covered by healthcare systems or insurance structures. These interventions create a direct link between food and health and are integrated into healthcare delivery.
Examples include medically tailored meals, medically tailored groceries, and produce prescription programs. Within this approach, food is not seen as an add-on, but as a core component of prevention and care.
For a concise overview, Tufts has published a Food is Medicine factsheet:
2. A rapidly growing evidence base
Dr Ridberg showed how the field has developed significantly in recent years. As of May 2025, more than 270 Food is Medicine studies have been published in peer-reviewed journals. The broader evidence base points in a consistent direction: these programs can improve food security and diet quality, are associated with better health outcomes, including weight, blood pressure, and HbA1c, and, in some cases, are linked to reduced healthcare utilisation and lower costs.
At the same time, the state of the evidence was not presented as overly optimistic. Dr Ridberg highlighted what is still needed: larger and longer-term studies, stronger implementation research, better economic evaluations, and more insight into what works, for whom, and under which conditions.
This combination of strong momentum and remaining questions makes this a particularly relevant moment to invest further in pilots, research, and system-level learning in the Netherlands.
3. Lessons from the U.S., but no one-size-fits-all model
The webinar included several examples from the United States related to financing and scaling. While these examples are valuable and inspiring, they cannot be directly replicated in Europe. Differences in healthcare systems, reimbursement structures, and food cultures are simply too significant.
Dr Ridberg emphasised this in the final part of her presentation on adaptation, highlighting the importance of local dietary habits, shared measurement frameworks, participant experience, and early alignment with healthcare systems.
For the Netherlands, the question is therefore not whether Food is Medicine exists elsewhere, but how these models can be adapted to a context where municipalities, health insurers, hospitals, researchers, and farmers all play a role.
4. Early alignment with healthcare systems is essential
One of the most practical insights from the session concerned implementation. If Food is Medicine is to become part of mainstream care, key elements must be considered early on: target populations, referral pathways, financing structures, training of healthcare professionals, and data collection.
Without this integration, food-based interventions risk remaining isolated pilot projects.
5. Local context determines success
Dr. Ridberg emphasized that Food is Medicine cannot simply be copied from one country to another. Programs must align with local healthcare systems, food cultures, and the everyday realities of participants.
For the Dutch context, this is a key insight: success depends not only on clinical outcomes, but also on accessibility, trust, and whether people can realistically integrate healthy food into their daily lives.
For the Dutch Food Pharmacy model, this means that impact is not only about biomarkers or reduced healthcare costs, but also about reach, feasibility, and long-term sustainability.
What changed for participants during the session?
The webinar clearly increased participants’ understanding of the topic. At the start, only 24% of respondents reported being familiar or very familiar with the Food is Medicine movement. After the session, this had risen to 64%.
Familiarity with Food Pharmacy models also increased significantly, with the share of participants who felt at least reasonably familiar growing from 26% to 62%.
Confidence in the model also improved. The percentage of respondents who believed that Food Pharmacy could have a strong or very strong impact on health outcomes increased from 68% to 83%. By the end of the webinar, 85% of participants saw moderate to strong opportunities for Food Pharmacy in their own region.
Connecting the Food is Medicine movement and AHOPM
The Agri-Health consortium is actively exploring how Food is Medicine models can be applied in the Dutch context. HarvestCare Foundation, the lead partner of the consortium, is already implementing a Food Pharmacy model in Rotterdam for people with diet-related conditions, including type 2 diabetes.
Within this model, participants receive weekly boxes of locally produced organic food as part of a food-as-medicine approach, with the broader goal of embedding nutrition as a medical intervention within the Dutch healthcare system.
This work builds on years of pioneering Food is Medicine programs in the United States and beyond, particularly producing prescription models that provide patients with access to healthy food as part of prevention and care. The consortium aims to build on this scientific foundation and program logic and translate it into the Dutch context. This includes adapting healthcare structures, financing mechanisms, local food environments, and the necessary partnerships to make these models viable in practice.
This is also where the connection with local and regenerative agriculture becomes crucial. If healthy food becomes part of healthcare, local and regenerative farmers are no longer peripheral suppliers, but part of the solution itself. The consortium’s ambition is not only to improve health outcomes, but also to create new demand for food produced in ways that support soil health, biodiversity, and long-term resilience.
At the same time, the consortium is part of a broader international Food is Medicine movement that works on scaling impact, sharing learnings across programs, and—where useful—aligning methodologies, while maintaining room for local adaptation. The Dutch work is therefore grounded in international knowledge and experience, but shaped for the Dutch reality.
Conclusion
This first webinar made it clear that Food is Medicine is no longer a niche. The field is maturing, the evidence is growing, and the central question is shifting from “does it work?” to “how do we organise and finance it effectively?”
AHOPM is operating within that same transition: connecting healthy food, improved health outcomes, fairer revenue models for farmers, and new approaches to financing prevention.

